
German excess mortality (Part 4)
A barkless hellhound is the New Kid on the Block

Update 2023-04-05


Summary
The CFR (case fatality rate) of COVID-19 in Germany increased from ~0.15% during the first half of 2022 to over 0.8% in late January 2023.
Mass deceptive immune imprinting with leaky vaccines allows new SARS-CoV-2 variants to gain predominance. This is confirmed by the correlation between the proportion of bivalently boosted individuals and the proportion of sequenced SARS-CoV-2 samples that were positive for the lineage BQ.1.1* (Pearson correlation coefficient = 0.60).
The recent increase in Germany’s COVID-19 CFR is owed to this lineage (BQ.1.1) which is fully adapted to escape the immunity provided by bivalent boosters.
The German COVID-19 hospitalization rate has been rising all throughout 2022 to reach a level of over 7% in the last calendar week. With such a high hospitalization rate I expect a lot of asymptomatic cases to have gone undiagnosed.
Since bivalent boosters are advertised as protecting from symptomatic disease, I propose that those variants well-adapted to the immunity provided by bivalent boosters can rapidly induce sudden death in bivalently boosted individuals, after a short asymptomatic disease course that often goes undiagnosed.
Bivalently boosted individuals have been rendered unable to produce any neutralizing antibodies against the variants BQ.1.1 and CH.1.1 which were mockingly named Cerberus and Orthrus by the WHO, after the three-headed hound guarding the gates of hell and his two-headed brother.
I am afraid we have not seen the last of COVID-19 just yet, but fortunately for us Pfizer is eager to protect us through their experiments in directed virus evolution. I write about my take on the Project Veritas leak in the Discussion section.
Recap
German excess mortality Part 1
The first article contains a large number of charts displaying mortality, trend-corrected mortality, average (seasonal) mortality and excess mortality figures of all federal lands for 2010-2022. These charts are well worth looking into if you want to gain an impression of the situation in Germany.

I concluded that German excess mortality in 2022 was not only exceptionally high, but also increased steadily throughout 2022 which is highly unusal.
German excess mortality Part 2
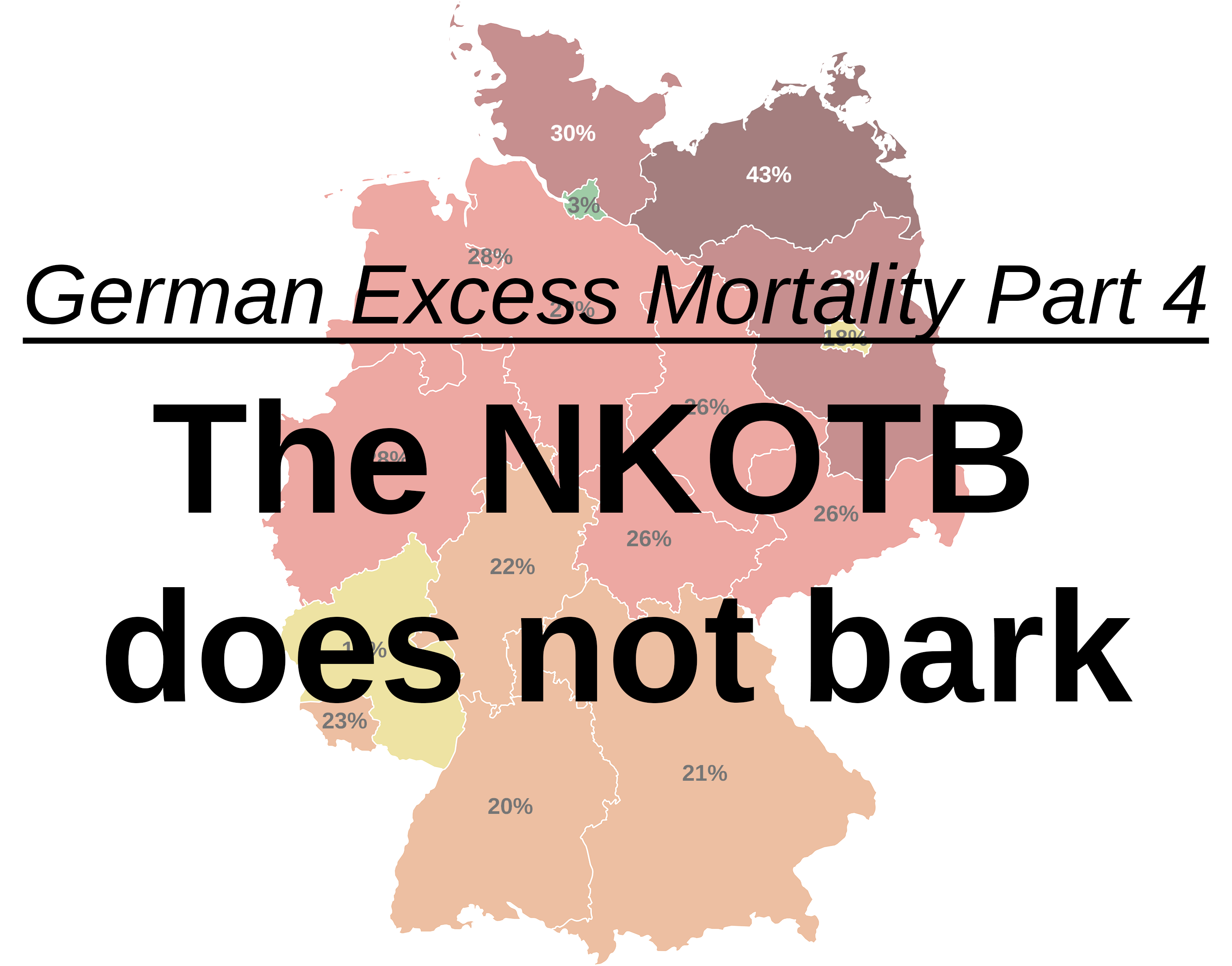
In the second article I looked at the net impact nucleotide-based COVID-19 vaccines had on mortality throughout 2021 and 2022.
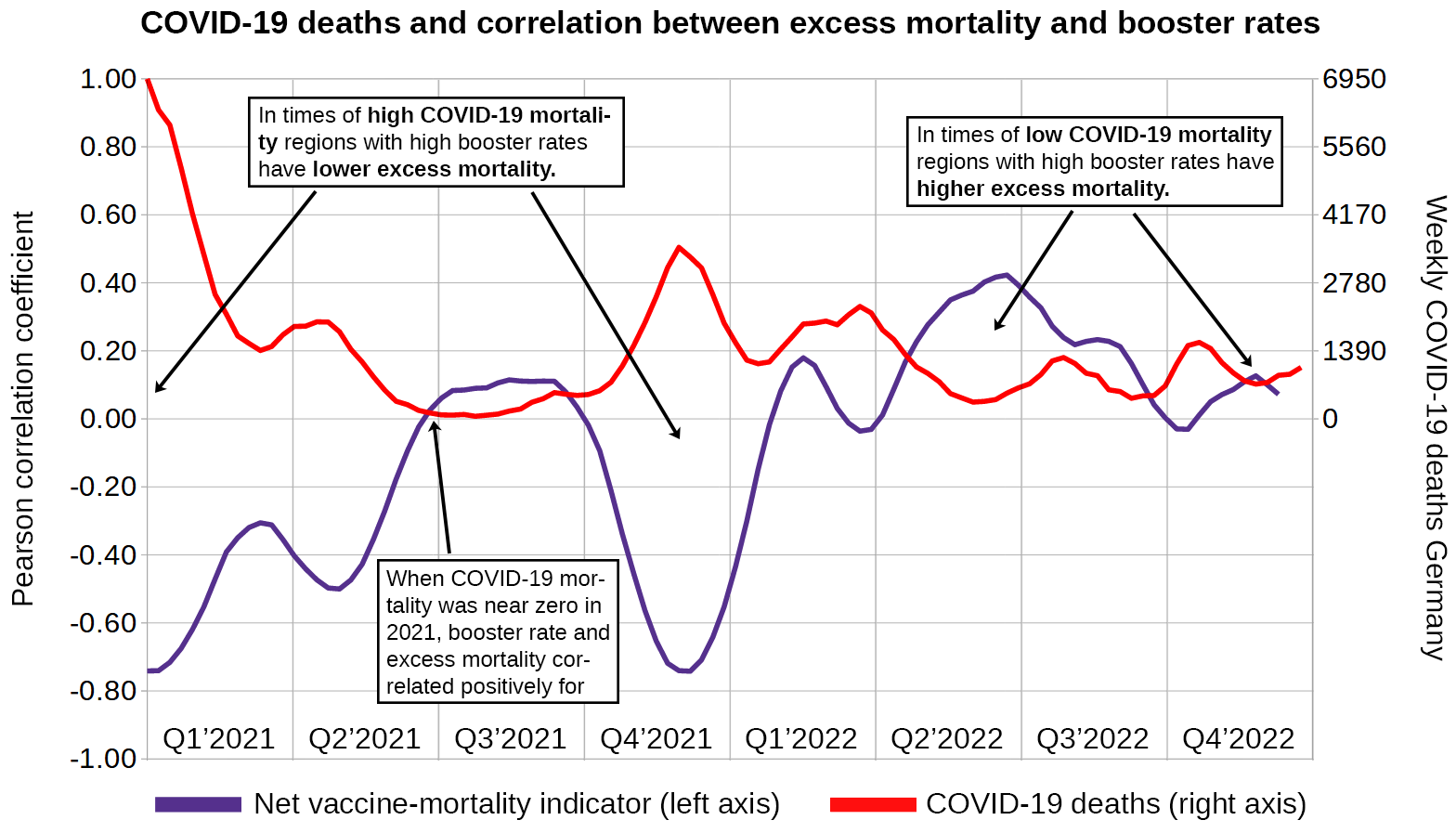
I plotted the Pearson correlation coefficient between excess mortality and vaccination rates across German federal states over the course of 2021-2022 and drew two conclusions:
Vaccines net impact reduced mortality in 2021
Vaccines net impact increased mortality in 2022
Federal states with higher vaccination rates see lower excess mortality during COVID-19 waves
Federal states with higher vaccination rates see higher excess mortality outside of COVID-19 waves
German excess mortality Part 3
I took a closer look at non-COVID excess deaths during the initial vaccination effort between week 8/2021 and week 27/2021 and found a very strong correlation between the weekly number of vaccine doses administered and the weekly number of non-COVID excess deaths on the national level (Pearson correlation 0.980) and in every of the 16 German federal states (Pearson correlation 0.893 - 0.981).

Based on this I concluded that every 1642 (95% CI: 1477-1808) administered COVID-19 vaccine doses cause one excess death.
Introduction
Welcome to part 4 of this series. Today I am looking at patterns of COVID-mortality throughout the year 2022.
According to RKI data only a small proportion of German excess deaths of 2022 are owed to COVID-19, but there is a worrying trend that suggests the CFR of COVID-19 has been increasing in recent times, possibly owed to the deployment of bivalent boosters.
Methods
CFR
I am using Our World in Data’s variable cfr_short_term for displaying the case fatality rate. Smoothed graphs represents a bidirectional moving average of 7 days.
Bivalent booster rates
Information about the proportion of people in each federal state who have received a bivalent booster is not made public and neither is the proportion of people who received their 3rd or 4th booster dose made public. The RKI is simply not releasing these data. It rests safely with the Bundesdruckerei GmbH, a German NGO that is responsible for issueing passports and identification cards.
Instead I am using the proportion of individuals aged 60+ who according to RKI figures have received their 2nd booster between September 7th 2022 and December 31st 2022, a time during which bivalent boosters were available.
Variant data
I calculate the proportion of each variant among sequenced SARS-CoV-2 samples by dividing the number of times it was sequenced per day by the total number of sequenced samples on the same day.
This number is then multiplied by the number of newly registered cases to yield the number of new variant cases. Every year is then stretched to 52 weeks.
To calculate the proportion of an entire lineage I add up the proportions of each variant that begins with the respective lineage’s name. For example the BQ* lineage contains the following variants:
BQ.1, BQ.1.1, BQ.1.1.1, BQ.1.1.10, BQ.1.1.11, BQ.1.1.12, BQ.1.1.13, BQ.1.1.15, BQ.1.1.16, BQ.1.1.17, BQ.1.1.18, BQ.1.1.19, BQ.1.1.2, BQ.1.1.20, BQ.1.1.21, BQ.1.1.22, BQ.1.1.23, BQ.1.1.24, BQ.1.1.26, BQ.1.1.27, BQ.1.1.28, BQ.1.1.29, BQ.1.1.3, BQ.1.1.31, BQ.1.1.32, BQ.1.1.34, BQ.1.1.4, BQ.1.1.5, BQ.1.1.6, BQ.1.1.7, BQ.1.1.8, BQ.1.10, BQ.1.10.1, BQ.1.11, BQ.1.12, BQ.1.13, BQ.1.13.1, BQ.1.14, BQ.1.15, BQ.1.16, BQ.1.17, BQ.1.18, BQ.1.19, BQ.1.2, BQ.1.20, BQ.1.21, BQ.1.22, BQ.1.23, BQ.1.24, BQ.1.25, BQ.1.26, BQ.1.26.1, BQ.1.28, BQ.1.3, BQ.1.4, BQ.1.5, BQ.1.6, BQ.1.8, BQ.1.8.2, BQ.2Excess mortality
I have discussed extensively how I think excess mortality should be calculated for this purpose in past articles of this series.
Hospitalizations, new deaths, new cases
These data are all stretched to 52 weeks per year.
COVID-19 deaths curve fitting
I do this manually from within a very basic spreadsheet written in LibreOffice.
Charts
Charts are generated with LibreOffice and post-processed with Adobe Photoshop.
Data sources
Downloads
Results
Excess mortality and COVID-19 mortality
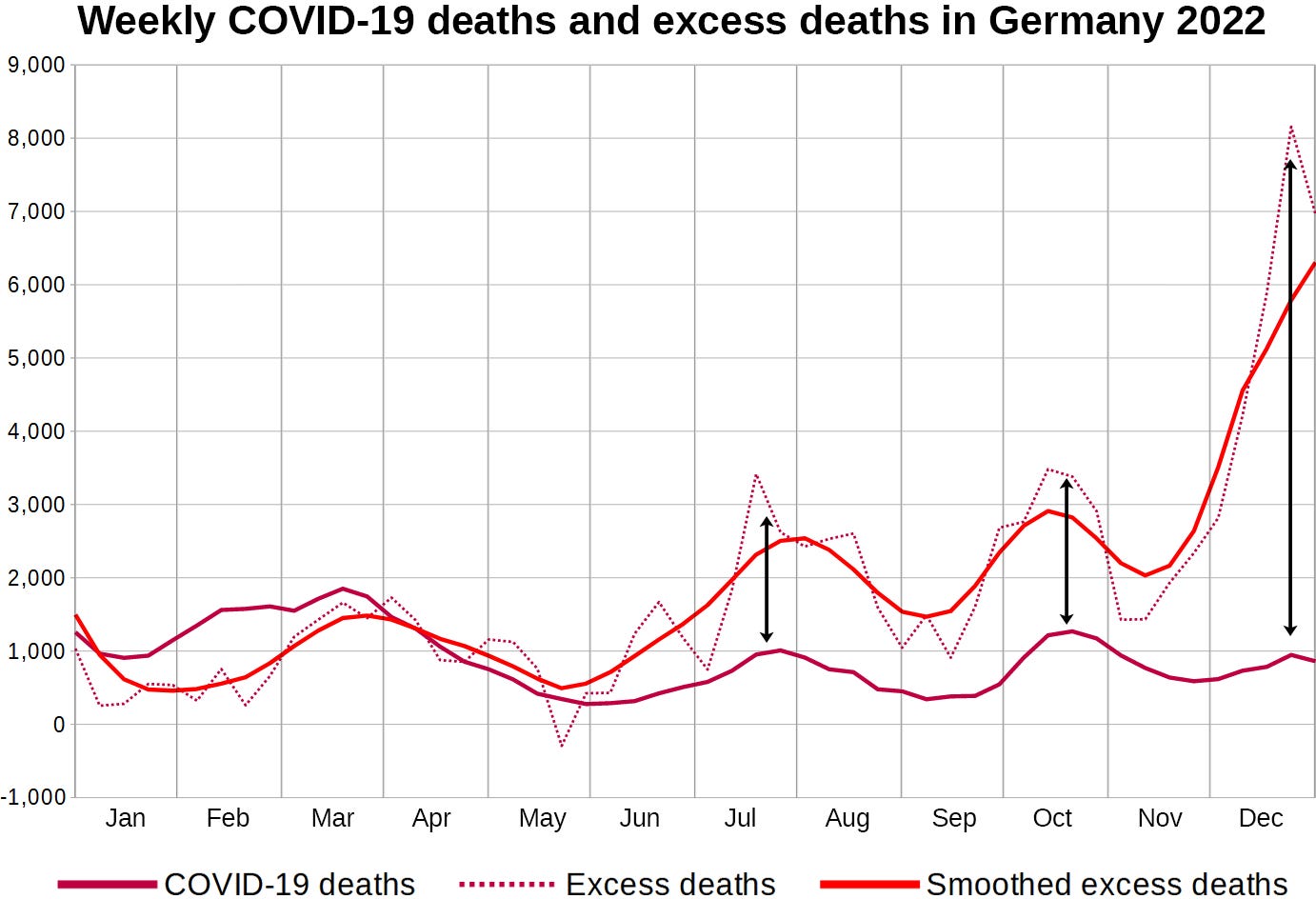
It looks like COVID-19 is only a minor factor in German mortality. However I find it remarkable how both curves seem to be synchronized.
It can not hurt to take a closer look at some related variables.
COVID hospitalizations
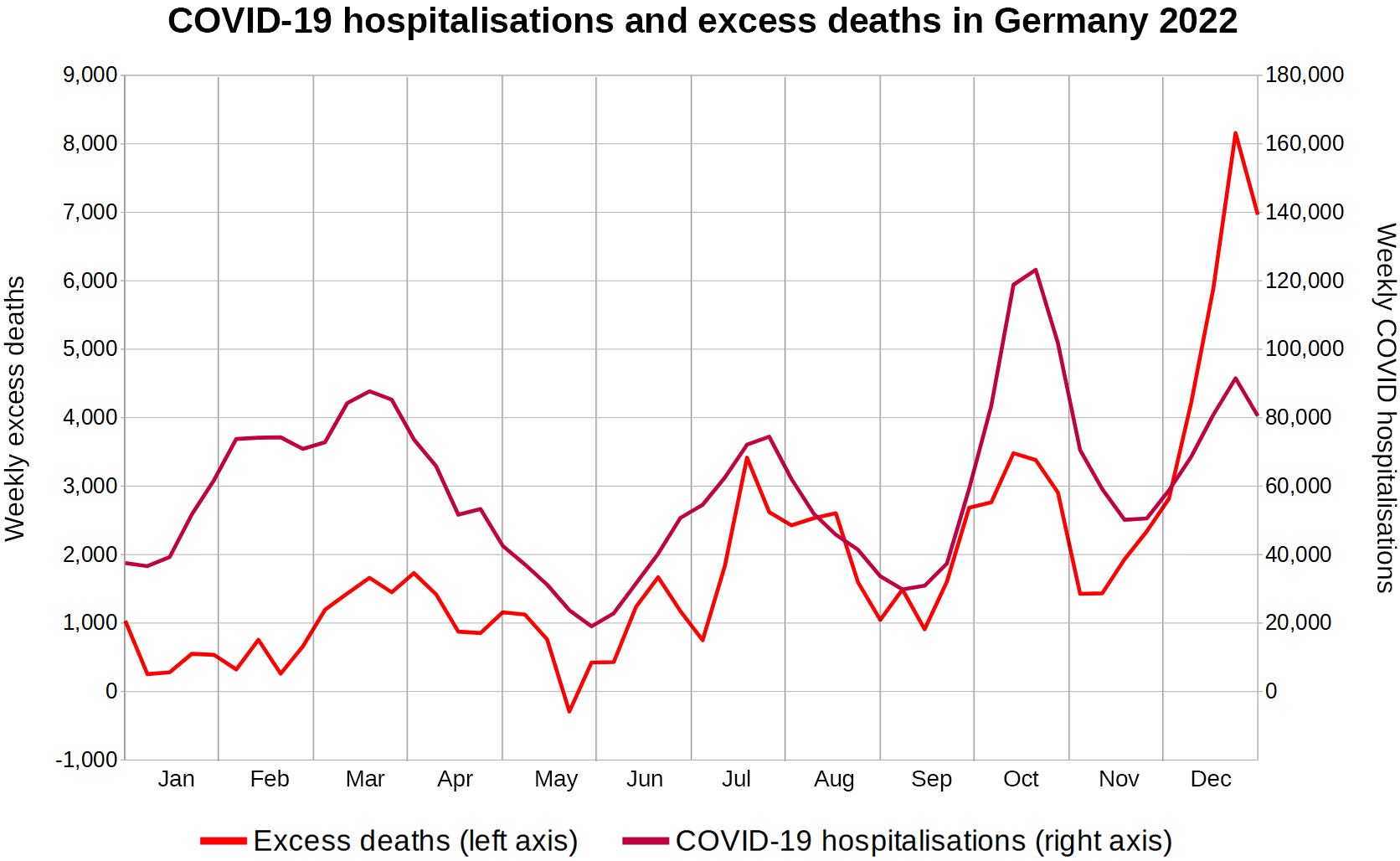
COVID hospitalizations harmonize equally well with excess mortality. It looks like COVID hospitalisations are seeing a steeper increase than COVID deaths, so I am plotting the number of registered COVID deaths per COVID hospitalization.

The number of hospitalisations per death has been increasing throughout 2022. This could indicate better disease management. Let’s take a look at the proportion of COVID cases that is being hospitalized.

According to these data, the proportion of COVID-19 cases that is being hospitalized has risen from 1% to 7% during the second half of 2022. This could indicate that the infection has become more dangerous or it could just indicate decreased testing efforts.
I’d have expected such a steep rise in the COVID hospitalization rate to be mentioned by major news outlets. Why have I not heard of this?
If hospitalizatios per case have been increasing much faster than hospitalizations per death, then the CFR must’ve been increasing as well.
The COVID-19 CFR is increasing
I looked at the CFR as specified by 'Our World in Data'.
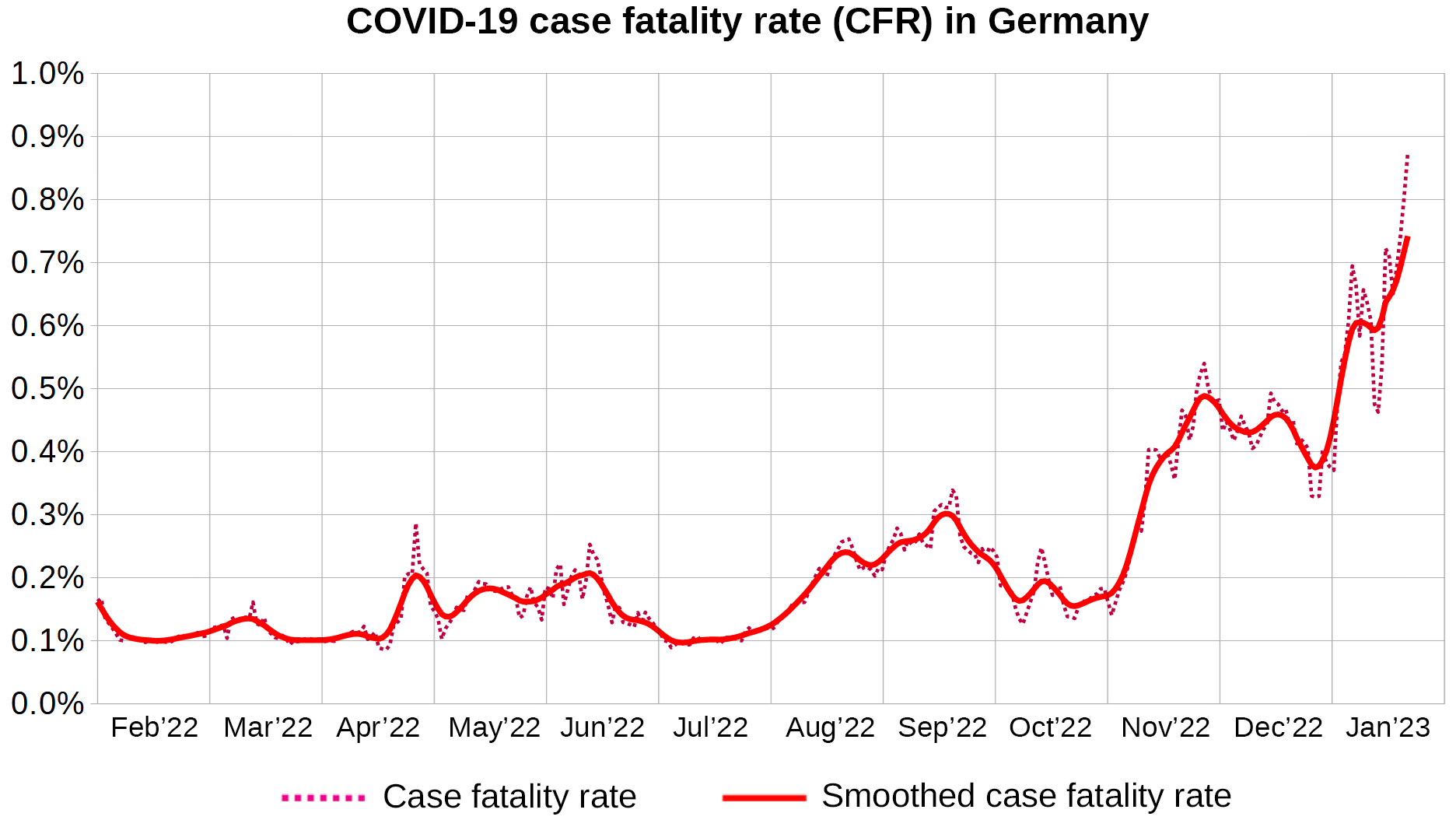
The CFR has indeed been increasing in a very similar manner to both the hospitalisation rate of COVID-19 cases and excess mortality.
I am plotting new COVID-19 cases next to new COVID-19 deaths.

Throughout 2022 the number of COVID-19 deaths per newly registered COVID-19 case has been increasing. This is reflected by the increasing CFR.
The last COVID-19 wave of 2021 was caused by the Delta variant which had a much higher CFR (case fatality rate) than the Omicron variants we saw in 2022.
In order to get a more detailled view of what is going on, I decided to take a closer look at the variants that are causing these waves.
New cases stratified by variant
I first identified variants that were predominant during late 2021 and 2022 and grouped them according to their lineage. The most common lineages were:
AY* (Delta): 184 variants
BA.1* (Omicron): 47 variants
BA.2* (Omicron): 127 variants
BA.5* (Omicron): 96 variants
BE*: (Omicron): 23 variants
BF*: (Omicron): 59 variants
BQ* (Cerberus): 60 variants
The proportion of each lineage among sequenced samples was applied to the total number of new cases each week. The resulting variable represents an estimate of the number of new weekly cases attributed to the respective variant.

To make sure I didn’t miss any major lineages I added up all new variant cases and compared them to the total number of new cases.

The seven lineages make up 96.7% of COVID-19 cases between July 1st 2021 and December 31st 2022. The gap in the third quarter of 2022 is made up by BA.4 variants and the gap towards the end of 2022 is made up BN* and CH* variants.
The lineages I picked should suffice to model COVID-19 mortality.
Modelling COVID-19 mortality
I started off by assigning a CFR of 1:1000 to each variant and then proceeded to manually adjust the CFR’s of all lineages until the modelled COVID mortality matched the COVID mortality data issued by the German government.

After shifting the predicted deaths by 1 week R-Squared is 0.92.
These are the CFR’s that I determined for each lineage:
0.71%: AY* (1 death per 140 cases)
0.12%: BA.1/BA.2/BA.5* (1 death per 850 cases)
0.25%: BE/BF* (1 death per 400 cases)
0.80%: BQ* (1 death per 125 cases)
The BQ* lineage seems to have a CFR slightly above that of Delta and roughly 6.7 times as high as that of Omicron.
Since BQ* is currently the predominant lineage in Germany we seem to be back to the Delta days in terms of case fatality rate.
Is this a consequence of bivalent boosters being deployed in September 2022?
Bivalent booster adapted strains
I wanted to find out whether or not bivalent boosters are to blame for BQ.1.1’s predominance, so I plotted the proportion of bivalently boosted 60+ year olds and the relative prevalence of BQ.1.1 onto a scatter chart and calculated the Pearson correlation.

The Pearson correlation coefficient is 0.60. This indicates a strong correlation between the relative prevalence of BQ.1.1 and the administration of bivalent boosters.
Out of curiosity I also checked on CH.1.1, which relative prevalence correlates moderately strong with the proportion of people who received bivalent boosters (Pearson = 0.38).
Discussion
New variants
Vaccinations with spike protein or vectors that induce spike protein are putting immense immune pressure on SARS-CoV-2 whenever vaccinated individuals become infected.
Since the vaccinations do not provide sterile immunity mutated virus particles forming within the bodies of vaccinated infected patients have plenty of opportunity to infect other patients.
The more people receive the same type of deceptive immune imprinting through vaccination, the larger the growth advantage of these newly evolved variants is and the more likely the variant is to gain predominance over other circulating variants.
While natural immunity should generally make a person well-equipped for fending off these new variants, the vaccine-adapted variants come with specially tailored capabilities for evading the humoral immunity of patients whose immune systems have been repeatedly imprinted with various versions of the spike protein that are not encountered in the wild anymore.
There are currently no vaccines that can provide humoral antibody immunity against the most recent SARS-CoV-2 lineages BQ.1.1 and CH.1.1. They can both escape all monoclonal antibody drugs except for SA55 and SA55+ which are still in an experimental phase.
It remains to be seen how these new variants affect the unvaccinated. Alas mortality data stratified by vaccination status is still very sparse more than two years into the deployment of modRNA drugs.
Directed evolution
Since I do not condone the way Project Veritas operates, I will not link to them directly. In one of their last episodes they secretely filmed Pfizer’s director of research and development bragging about how Pfizer is developing new variants.
This is what I think the Pfizer employee is talking about when he is referring to directed evolution:
If you embrace the hypothesis that these modRNA drugs are allowing new variants to gain predominance, you will easily be able to smell the business opportunity in knowing the sequences of emerging variants before they pop up in the wild.
All you have to do in theory is administer the latest vaccine to a group of primates, infect them with the currently predominant SARS-CoV-2 strains and sequence a sample after a period of delay during which the virus has time to adapt.
Pfizer executives seem to believe, that if they had done this with the BA.4/BA.5 vaccine, they might have been able to anticipate BQ.1.1 to start work on the next update early.
While this may seem deeply immoral, the real issue at hand is that these vaccine-adapted variants are gaining predominance in the first place.
Both the responsible Pfizer executives and their drugs need to be stopped.
Impact on excess mortality
According to official figures only 19,675 of the 73,217 excess deaths (27%) that occurred in the second half of 2022 were attributed to SARS-COV-2.
My gut says the remaining excess mortality is owed to vaccines. However even in times when excess deaths far exceed COVID deaths like they did during the last 3 weeks of 2022 both time series are still in sync.
The relationship between COVID-19 waves, vaccinations and excess mortality may be more complex yet.
Do barkless dog breeds bite harder?
SARS-CoV-2 and COVID-19 modRNA vaccines are different vectors carrying the same payload. The spike protein seems to be the pathogenic element that allows both virus and vaccines to cause disease in very similar ways.
We know various mechanisms by which immune tolerance can develope after repeated exposure to spike protein:
The vaccines are currently advertised as preventing symptomatic disease.
Symptom
a physical or mental feature which is regarded as indicating a condition of disease, particularly such a feature that is apparent to the patient.The most common COVID-19 symptoms that the vaccines “protect” from by order of frequency are cough, pyrexia, fatigue, headache, dyspnea, chills, nausea, diarrhoea, rhinorrhoea.
Symptoms are what motivates a person to take a test.
However other aspects of SARS-CoV-2 associated disease do not necessarily produce any symptoms. Among them are cardiac arrhythmias, coagulopathies and sudden death.
With the steep increase in CFR and a hospitalization rate of over 7%, undiagnosed cases could account for some of the excess deaths.
I hypothesize that mass deployment of bivalent boosters has turned SARS-CoV-2 into a silent killer of the bivalently boosted.
VAERS
I have seen correlations between decreased symptom severity and increased proportions of coagulopathies and deaths in Delta and Omicron associated VAERS adverse event reports and will try to dedicate an article to this in the future. The data is highly complex due to the varying degree of variant prevalence over time.
An additional dose series increases immune tolerance and at the same time the patients will encounter different variants depending on the time of vaccination and the time of symptom onset, as specified in the reports. All these aspects have a strong influence on symptom proportions.

The Schadenfreude of the WHO
It is noteworthy that the WHO mockingly named BQ.1.1 Cerberus and CH.1.1 Orthrus.
Cerberus is the three-headed hound that is guarding the gates of hell and Orthrus is his two-headed brother.
A German team of researches once referred to COVID-19 as a “Three-Headed Cerberus” of inflammation, coagulation and destruction.
Both variants have in common that the bivalently boosted can not produce any neutralizing antibodies against them.
Conclusion
The overall CFR (case fatality rate) of COVID-19 in Germany increased from ~0.15% during the first half of 2022 to over 0.8% in late January 2023.
Mass deceptive immune imprinting with leaky vaccines allows new SARS-CoV-2 variants to gain predominance. This is confirmed by the correlation between the proportion of bivalently boosted individuals and the proportion of sequenced SARS-CoV-2 samples that were positive for the lineage BQ.1.1* (Pearson correlation coefficient = 0.60).
The recent increase in Germany’s COVID-19 CFR is owed to this lineage (BQ.1.1) which is fully adapted to escape the immunity provided by bivalent boosters.
The German COVID-19 hospitalization rate has been rising all throughout 2022 to reach a level of 7% in the last calendar week. With such a high hospitalization rate I expect a lot of asymptomatic cases to have gone undiagnosed.
Since bivalent boosters are advertised for protection from symptomatic disease, I propose that those variants well-adapted to the immunity provided by bivalent boosters can rapidly induce sudden death in bivalently boosted individuals, after a short asymptomatic disease course with a tendency to go undiagnosed.
Bivalently boosted individuals have been rendered unable to produce any neutralizing antibodies against the variants BQ.1.1 and CH.1.1 which were mockingly named Cerberus and Orthrus by the WHO, after the three-headed hound guarding the gates of hell and his two-headed brother.
I am afraid we have not seen the last of COVID-19 just yet, but fortunately for us Pfizer is eager to protect us through their experiments in directed virus evolution.
Great post Fabian. Very much fitting my yesterday's story.
It is also highly disturbing as to its implications.
It is also upsetting just how much the authorities want to suppress this information.
Do you want to exchange large format links?
Great work as usual. If you can stand it, I am pretty sure your skills are in high demand in investment management, banking or consulting for risk adjusted performance attribution and ex-ante risk modelling!
I confess I did some mental gymnastics when I read "If hospitalizatios per case have been increasing much faster than hospitalizations per death, then the CFR must’ve been increasing as well."
Mentally, I eliminated "hospitalizations" from the sentence and arrived at cases/deaths = CFR - which, of course is the inverse of the CFR (deaths/case, usually expressed as deaths per 100k or 1m cases)!
good to see igor active on your thread. not that I am the third head of our own cerberus!
i posted on his stack that the spike protein is the key that unlocks a kraken - whether that is from sars-cov2 virus or from the body making it post injection.
In my (layman's) world - I would be seeing how to put the kraken back in the cage using prison bars made of IgG1 and 3 antibodies, plus using IVM/HCQ/steroids/melatonin protocols as a crude adobe prison cell until i could figure out how to make a maximum security facility!
anyway, hats off to you. very worrying developments (geert was right, it looks like - we might be running into a next variant which is more infectious AND more deadly than any we hve seen thus far.