
The underreporting factor is 1073
for incidents of any type occuring within 7 days after dose 1

Summary
In this article we will find out that headaches occuring within 7 days of receiving the first dose of a modRNA vaccine have been underreported by a factor of 1280, from which we infer that all incidents occuring within 7 days of dose 1 of a modRNA vaccine have been underreported by a factor of 1073.
Introduction
Many articles have been written about the URF (underreporting factor), most notably by Jessica Rose and Steve Kirsch. I personally do not think that the URF itself is of much interest, because it varies immensely between medical concepts. It is a dead end. Yet, I want to clear up some things about it.
We can determine the URF for specific symptoms that are representative for the overall adverse event reporting behaviour of patients. Headaches are such a representative symptom.
Methods
In my last article we learned that the 7 day incidence proportion for headaches occuring within 7 days of receiving dose 1 was roughly the same as the proportion of reports that mention the MedDRA term “Headache” among those reports about adverse events occuring within 7 days of receiving dose 1 of a modRNA vaccine.
This equiproportional relationship tells us that the proportion of headache incidents that is being reported is close to the proportion of adverse events that is being reported.
Hence, the URF for headache is close to the overall URF. So we are going to determine the URF for the MedDRA medical concept “Headache”.
We are going to compare the absolute number of headaches that occured within 7 days of dose 1, extrapolated from the results of a literature review with the absolute number of reports mentioning the concept among reports for that timeframe and dose number.
From the headache URF we will then infer the overall URF by looking at the ratio between report proportion and incidence proportion by applying what academics call the “rule of three”.
Results
The 7-day incidence proportion of headaches was determined to be 22% by an Italian literature review.

According to Bill Gates’ and Susanne Klatten’s co-project Our World in Data 266.58mio Americans had received their first dose by October 27th 2022 (Figure 1).
A rate of 22% means 58,647,600 people experienced headaches within 7 days after their first dose:
x = n * p = 266,580,000 * 22% = 58,647,600
A VAERS search for adverse events that occured within 7 days after dose 1 resulted in 45,828 hits for the term “Headache” across 248,526 reports, which comes out to a report proportion of 18.44% (95% CI: 18.29-18.59%).
With 45,828 reports filed by November 4th 2022 that contain the term “Headache”, this means:
URF[headache] = x[incidents] / x[reports] = 58647600 / 45828 = 1279.7
Since we determined the report proportion of headache (18.44%) is different from the incidence proportion determined in the review (22%), we can infer the overall underreporting factor from their ratio, which should put it below the URF for headaches:
URF = URF[headache] * p[reports] / p[incidents]
URF = 1279.7 * 18.44% / 22% = 1073
The underreporting factor for any type of incident occuring within 7 days of the first dose of a modRNA vaccine is 1073.
Similarly we can calculate the URF for events occuring after the second dose of these cardiotoxic drugs:
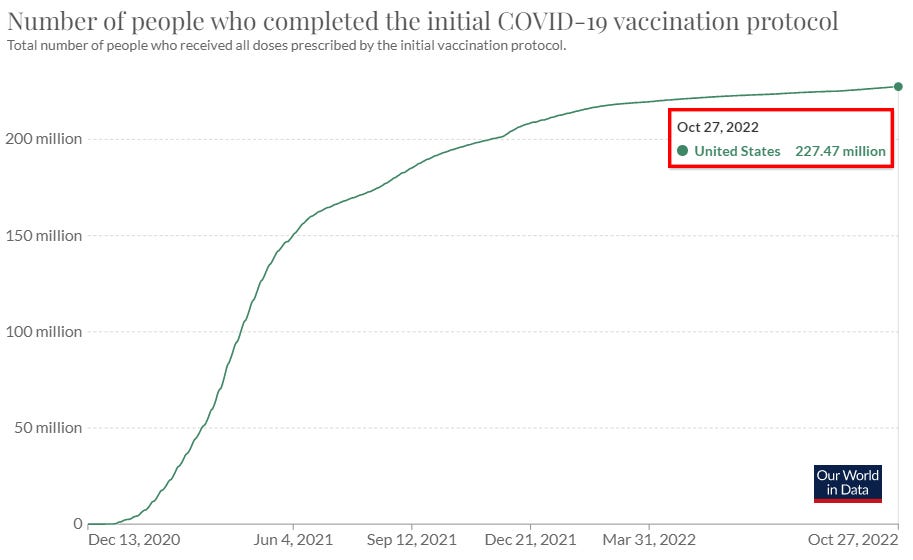
According to Our World in Data 227.47mio Americans had received their second dose by October 27th 2022 (Figure 2).
At a rate of 29% 65,966,300 people experienced headaches within 7 days after their receiving their 2nd dose.
We previously found out that these are represented by 37,052 hits across 154,175 reports. Therefore:
URF[headache] = n[incidents] / n[reports] = 65966300 / 37052 = 1780.4
URF = 1780.4 * 24.03% / 29% = 1475
So it seems the the proportion of adverse events occuring within 7 days of drug administration that is reported to VAERS is lower for the second injection that it is for the first which makes sense from a behavioural perspective.
Discussion
What can we do with these 7-day--underreporting factors? For general symptoms, which can be expected to have a report proportion similar to their incidence proportion, we can use it to estimate the absolute number of events that occured within seven days after being dosed.
If we have more data from literature, we can also use this knowledge to infer underreporting factors from other symptoms for additional timeframes.
However all of this will only take us so far. Underreporting factors should not be our primary concern. Instead we should focus more on report proportions for other general symptoms (opposed to more complex medical concepts) since these - as we have learned in my second article - often line up with the respective incidence proportions.
Report proportions are what give us an idea of the side effects profile. The underreporting factor gives us an idea of the magnitude of the the vaccination campaign’s impact on people.
In my fourth article, we will be looking at myocarditis associated symptoms and infer how many children had their hearts broken by the lies their governments had told them.
I've looked at URFs for deaths (https://www.trialsitenews.com/a/underreporting-factors-for-vaers-are-vastly-underreported-e3a21062). They are larger than most analysts have shown, and have been derived from the relatively short-term data we have accumulated so far. The long-term consequences of these shots could increase the death URFs substantially.