
How many children had their hearts broken?
It will break mine to tell you.

Summary
Today we are looking at the report proportion of the MedDRA term Chest pain for two different age groups to estimate how many children suffered heart injury within a week of receiving a COVID-19 vaccine.
We will find out that cardiac injury is a very common side effect among boys receiving their 2nd dose, while it is merely a common side effect among girls receiving their 2nd dose.
Introduction
To understand this article, you should have read my previous articles:
Are the modRNA vaccines enhancing SARS-COV-2 associated disease?
This is my first article which tackles the questions if a SARS-COV-2 infection increases the rate of cardiac injury in vaccinated children and if the unvaccinated suffer the same fate. It is not required reading.
Translating report proportions to incidence proportions
In the article before last we found out the incidence proportions of plain symptoms are often very close to the report proportions of the MedDRA terms that describe them.
The underreporting factor is 1073
In my last article we determined an underreporting factor of 1073 for events occuring within 7 days of receiving the 1st dose and an underreporting factor of 1475 for events occuring within 7 days of receiving the 2nd dose.
Methods
After determining the proportion of adverse events that mention “Chest pain” among reports about adverse events occuring within 7 days after administration of the 2nd dose, we will try to estimate what proportion of those events can be attributed to myocarditis caused by the COVID-19 vaccine and apply the 7-day-dose-2 underreporting factor to determine the incidence proportion of children suffering myocarditis within 7 days after receiving their second dose.
We will be looking at the report proportions for terms representing myocarditis-associated symptoms:
among two different VAERS report subsamples:
study group:
Reports about individuals who received 2 doses of a COVID-19 vaccine
reference group:
Reports about individuals who received any vaccine other than those intended to immunize against monkeypox (TYPE=SMALLMNK), smallpox (TYPE=SMALL, known to cause myocarditis) or COVID-19 (TYPE=COVID19)
We will be comparing working age adults (18-65) to children age 12 or older (12-17).
All eligible reports either have their age fields populated by the CDC or the age was parsed by running a Regular Expression on the narrative field:
/\W(\d{1,3})\W*ye*a*rs*\W*old$/i
Reports which age is neither specified nor can be parsed were excluded from the search.
Results
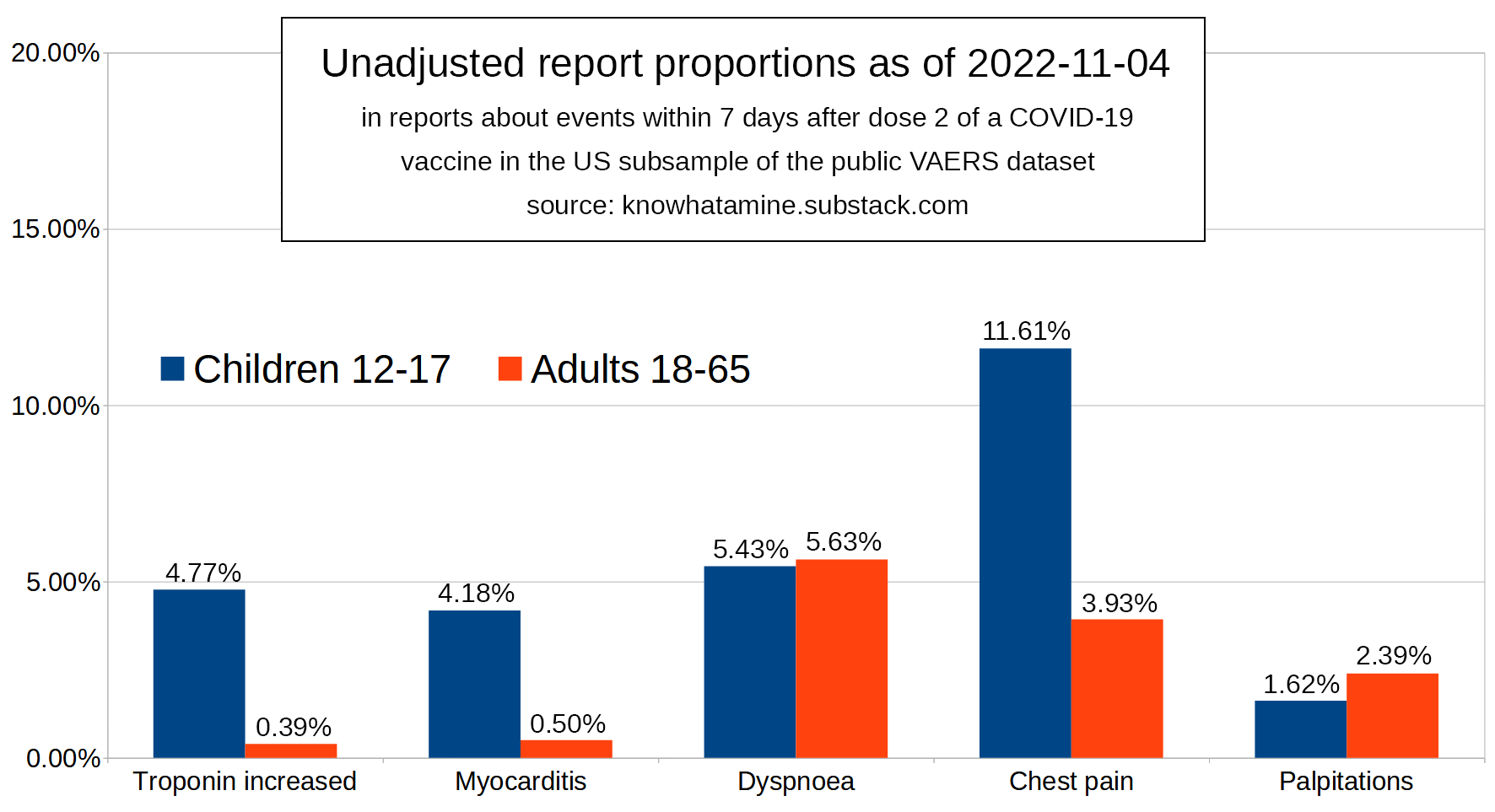
Looking at the results of our study report group in Figure 1 we can gather the report proportions containing each of the 5 terms both among reports about working age adults, as well as among reports about children in puberty.
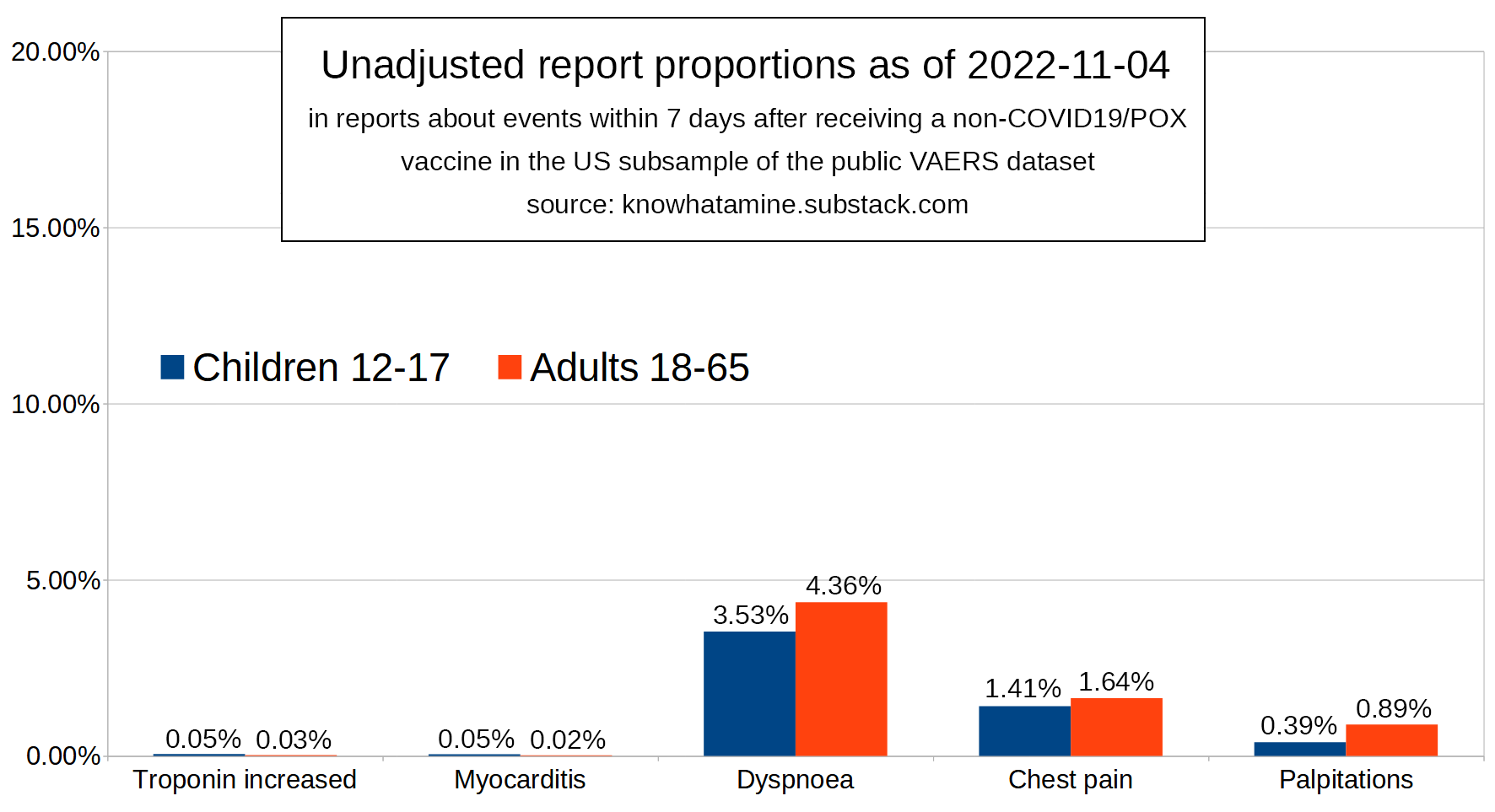
In Figure 2 we can see the report proportions for the same terms and subsamples in our reference report group. For each concept we now calculate the proportional reporting difference by subtracting the proportions in our reference group from the respective proportions in our study group.
This is expected to eliminate the proportion of events that is falsely attributed to the vaccine.
The result of this process can be seen in Figure 3 from which we can calculate proportional reporting ratios.
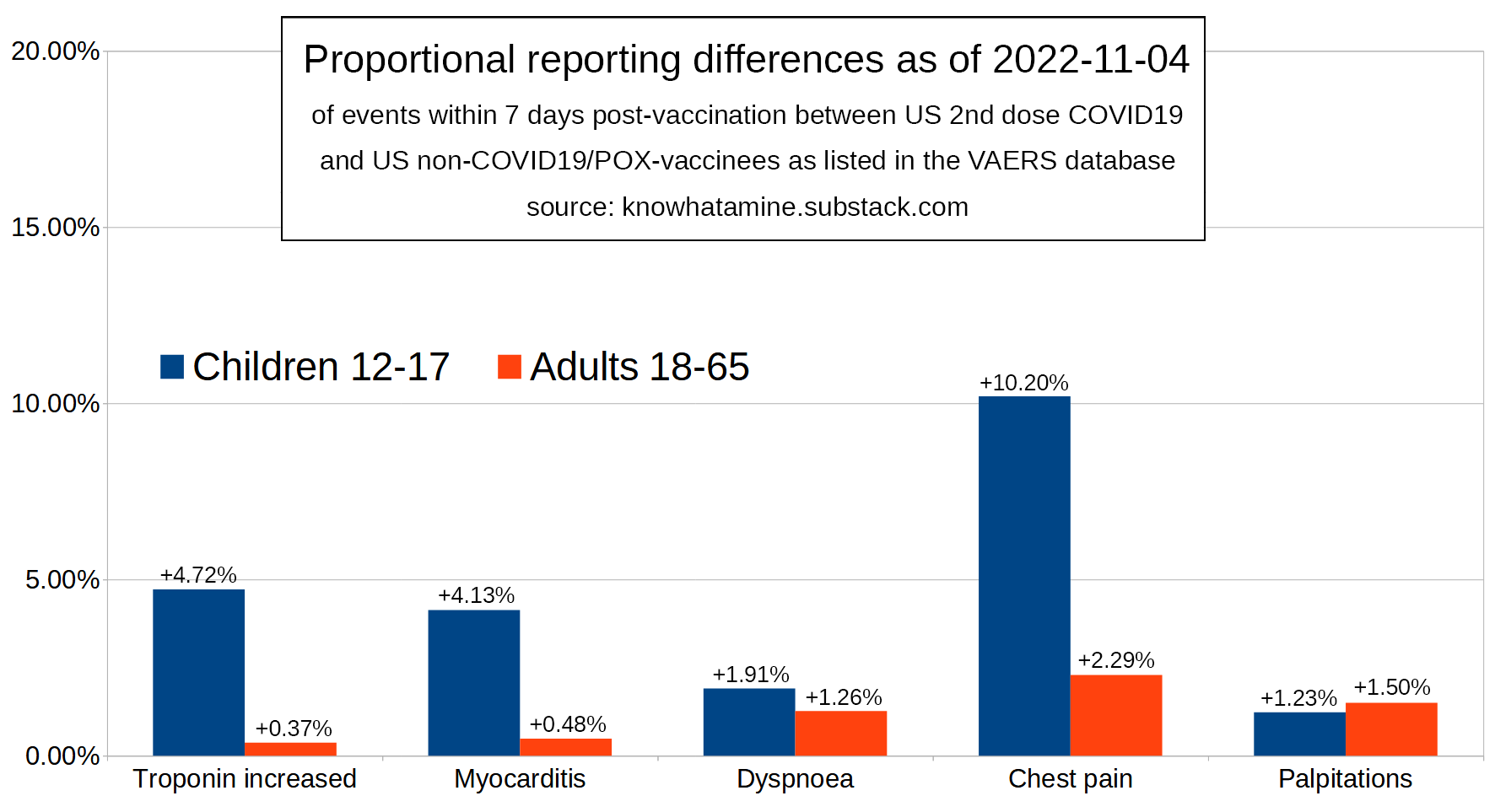
The proportion ratios between adults and children are:
12.14:Troponin increased8.34:Myocarditis0.97:Dyspnoea2.96:Chest pain0.68:Palpitations
From this and we can deduce the following assumptions:
“Troponin increased” and “Myocarditis” which are pathognomonic for cardiac injury occur much more frequently in reports about children than they occur in reports about adults (average PRR: 10.24)
“Dyspnea” or “Palpitations” alone are not an indicator of myocarditis
“Chest pain” indicates myocarditis with moderate specificity, since it is a leading symptom of myocarditis and generally occurs more frequently in adults (Figure 2), but more frequently in children in the case of COVID-19 vaccines (Figure 3).
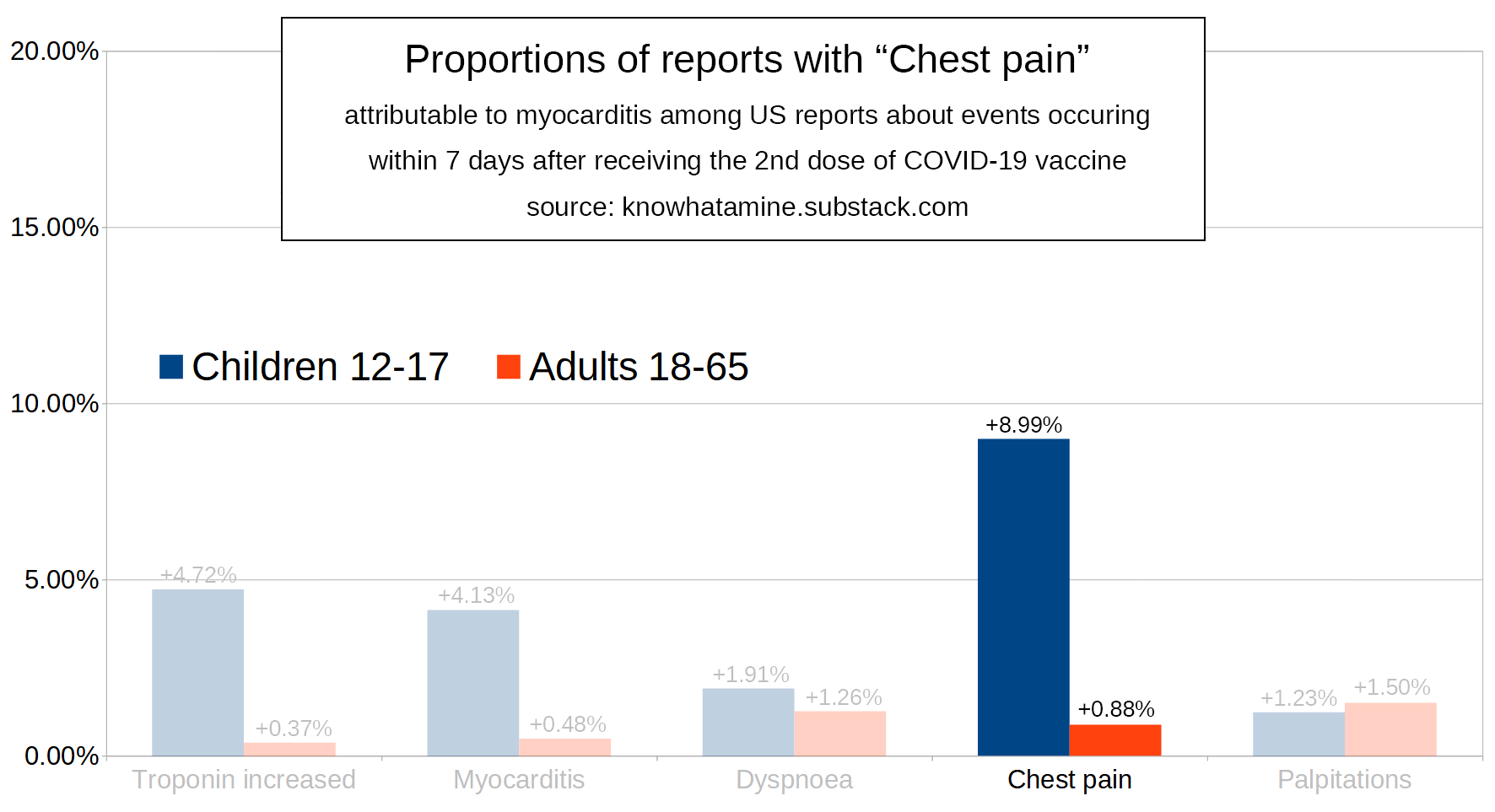
So now we will try to determine what proportion of events mentioning “Chest pain” is not attributable to pathophysiological processes other than myocarditis.
For this we will remove events from both adults and children that mention “Chest pain” until the “Chest pain” age group PRR matches the one of “Troponin increased” and “Myocarditis” (10.24).
This involves some simple math. We are trying to find the attributable proportions ac & aa, by determining and subtracting the deductable proportions dc & da from the report proportions pc & pa.
We want our final age-PRR to match that of “Troponin increased” and “Myocarditis”:
(1) ac = 10.24 * aaWe want the ratio of deductable proportions to match the age-PRR in our reference group:
(2) dc = da * 1.41% / 1.64%Our attributable proportions will be:
(3) ac = 10.20% - dc(4) aa = 2.29% - daNow we just fill in the values for
acanddcfrom the equation 1 and 2 into equation 3:10.24 * aa = 10.20% - da * 1.41% / 1.64%In order to be able to solve for the deductable proportion for adults
dawe fill inaafrom equation 4.10.24 * (2.29% - da) = 10.20% - da * 1.41% / 1.64%da = -1.2939% / -0.9160 = 1.41%We use
dato calculatedc:dc = da * 1.41% / 1.64% = 1.41% * 0.8598 = 1.21%And finally we calculate
ac = pc - dc = 10.20% - 1.21% = 8.99%aa = pa - da = 2.29% - 1.41% = 0.88%
Now we estimate the number of children who experience myocarditis-associated chest pain within one week of their second dose via two different methods:
We look at the number of reports about events in childrens of age 12-17 returned from our search, apply the report proportion of 8.99% and multiply this number with the 7-day-dose-2-URF estimated in my last article:
x = n * p * URF_2_7 = 7,105 * 8.99% * 1475 = 942,141We look at the number of children vaccinated and multiply this number with the report proportion which we assume to be approximately equal to the incidence proportion:
x = n * p = 15,100,000 * 8.99% = 1,357,490
Therefore we estimate the number of American children between 12 and 17 to have suffered cardiac injury within a week after being administered the 2nd dose of the COVID-19 vaccines to be between 0.94mio and 1.36mio.
In other words:
The proportion of children suffering cardiac injury within a week after being administered the 2nd dose of the COVID-19 vaccines is probably somewhere in the range between 9% and 11%.
Discussion
Statisticians will probably tell you this is all a load of bollocks. It’s not. I may not be a statistician and I may approximate and estimate a whole lot, but you can be dead certain: If I’ve ever done one thing right in my life it’s estimating stuff.
I estimate the true 7-week-dose-2 incidence proportion for cardiac injury to be larger than 9%, because…
…I expect the underreporting factor for children to be smaller than the one for adults.
…headaches are underrepresented (their report proportion is smaller than their incidence proportion), so I expect chest pain to also be underrepresented.
Between 9% and 11% may sound like a wide margin. It’s not. Right now the CDC is still telling us that myocarditis is a rare side effect. Rare means between 1 out of 1,000 and 1 out of 10,000 patients experience the event in question after receiving a drug.
For girls cardiac injury may still be a common side effect of the second dose which means between 1 out of 10 and 1 out of 100 girls’ hearts suffer are injured, but for boys it is a very common side effect of the second dose.
This means more than 1 out of 10 boys’ hearts are injured within a week after their 2nd dose of a modRNA COVID-19 vaccine.
So the CDC is giving us the wrong idea when they are saying it is a rare side effect. In my next article we will find out whether they are lying to us or are just clueless.
And before you mention that “incidence proportions are not report proportions”, I will stop you in the tracks to answer: They’re close enough
Conclusion
While cardiac injury seems to occur in more than 1/10 fully vaccinated boys and more than 1/100 fully vaccinated girls above 12, the CDC is still making claims of cardiac injury occurring in less than 1/1000 children.
Around a million American children between the ages of 12 and 17 have suffered cardiac injuries as a result of fulfilling government recommendations.
Notes
Never lose your humor in these darkest of times. I dare you to listen to this song. While you do that, look at these links to the relevant symptoms on pervaers.com:
Why did they have to run their game on us?
We should’ve known right from the start they’d go and break our hearts.
I'd love to review your method but it's been decades since my statistics studies. Maybe someone more fresh can do it.
https://www.youtube.com/watch?v=hQvTLtz67wM
World Government Summit 2022: What Pippa Malmgren is talking about is BLOCKCHAIN and digital currencies
“We are on the brink of a dramatic change where we are about to, and I’ll say this boldly,
we are about to abandon the traditional system of money and accounting and introduce a new one. And the new one; the new accounting is what we call blockchain…
It means digital, it means having an almost perfect record of every single transaction that happens in the economy, which will give us far greater clarity over what’s going on.”
Yes, because they do it for other purposes than health, very different purposes
https://outraged.substack.com/p/so-those-criminals-just-added-this
https://outraged.substack.com/p/world-government-summit-2022